El cáncer gástrico es un término general con el que se denomina a cualquier tumor maligno que surge de las células de alguna de las capas del estómago. Es la neoplasia más frecuente del tubo digestivo en todo el mundo, siendo la tercera causa de muerte por cáncer a nivel mundial en ambos sexos. El término cáncer gástrico se refiere a los adenocarcinomas del estómago, tipo histológico más frecuente, que representan un 95% de los tumores malignos de este órgano. Salvo en Japón, el carcinoma del estómago en general se encuentra en una fase evolutiva avanzada en el momento del diagnóstico, con infiltración más allá de la submucosa e invasión de la pared gástrica.
Cáncer Gástrico y su Tratamiento
¿Qué es el cáncer Gástrico?
FACTORES DE RIESGO
Son los agentes o condiciones que predisponen o aumentan las probabilidades de tener una determinada enfermedad.

FACTORES NUTRICIONALES: Dietas ricas en sal y ahumados típicas de Japón, Corea y China, bajas en frutas y en verduras frescas, y las concentraciones altas de nitratos en los alimentos favorecen el riesgo.
FACTORES AMBIENTALES: La mala preparación de los alimentos, la falta de refrigeración y las aguas en mal estado que pueden tener altas concentraciones de nitratos o de Helicobacter pylori aumenta el riesgo.
TABACO: El tabaco aumenta el riesgo de desarrollar muchos cánceres, incluido el de estómago.
ENFERMEDADES O CONDICIONES PREDISPONIENTES: La Enfermedades o condiciones predisponentes:
Cirugía gástrica previa: Han de trascurrir años para que aparezca un cáncer sobre el estómago residual (muñón gástrico). En general, este periodo suele ser superior a 10 -15 años.
Gastritis crónica atrófica: Puede ir degenerando hasta transformarse en cáncer.
Anemia perniciosa: Es un tipo especial de anemia, que aumenta el riesgo en unas 20 veces.
Pólipos gástricos: El riesgo de que se desarrolle un cáncer sobre un pólipo depende, entre otros factores, del tamaño del pólipo y de su histología. En general, a mayor tamaño, mayor riesgo de que se malignice.
Infección por H. Pylori: H. pylori es una bacteria que puede encontrarse en el estómago y causar úlceras y gastritis crónica. A nivel mundial es el factor de riesgo más importante del cáncer gástrico. Sin embargo, a pesar de aumenta el riesgo de cáncer gástrico, la mayoría de las personas con esta infección NO la desarrollará.
El reflujo gastro-esofágico: Aumenta el riesgo del cáncer de la unión gastro-esofágica.
Factores Familiares
DIAGNÓSTICO
El diagnóstico del cáncer gástrico se basa en la historia clínica, la exploración física, análisis de sangre, las pruebas de imagen como el TAC, la endoscopia digestiva alta (gastroscopia) y la biopsia.

CLÍNICA
ASINTOMÁTICO: El cáncer gástrico puede no producir síntomas hasta fases avanzadas.
La inversión reciente del pezón escamación, desprendimiento de la piel, formación de costras y pelado del área pigmentada de la piel que rodea el pezón (areola) o la piel de la mama, Enrojecimiento o pequeños orificios en la piel que se encuentra sobre tu mama, como la piel de una naranja.
SÍNTOMAS: Los síntomas (lo que nota el paciente) suelen ser vagos e inespecíficos. Los más frecuentes son indigestión, pérdida de peso, dolor abdominal en la parte superior, cambios en la frecuencia intestinal, pérdida de apetito y hemorragia digestiva. Las hemorragias pueden ser de varios tipos y causar anemia. También pueden notarse náuseas y vómitos, sensación de plenitud precoz (sensación de estar lleno después de comer poco) por falta de distensión de la pared gástrica, ascitis (acumulación de líquido en el abdomen), cansancio, etc
TRATAMIENTO
Resección endoscópica de la mucosa (REM): Esta técnica REM consiste en extirpar el tumor mediante gastroscopia y se reserva para cánceres que son en estadios iniciales.
A continuación, el detalle de algunas de estos tratamientos:
CIRUGÍA: La gastrectomía es la técnica quirúrgica estándar para resecar el tumor primario.
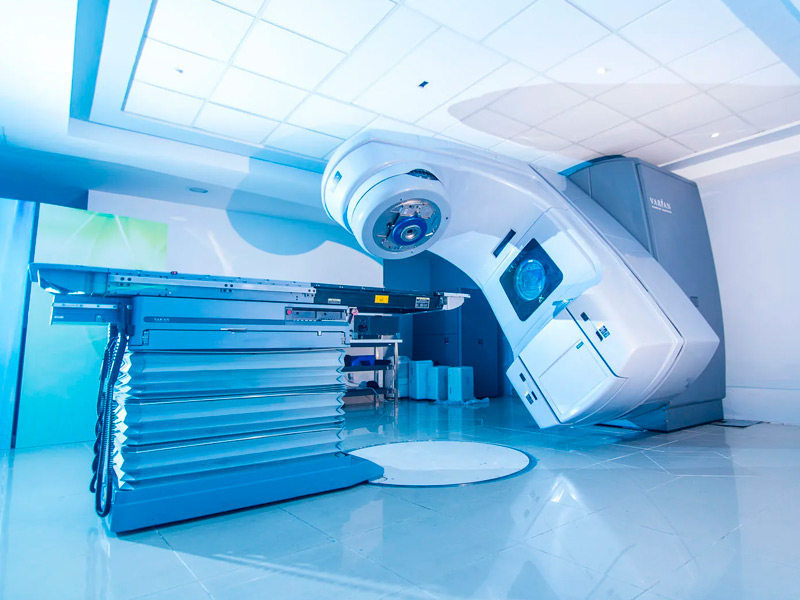
RADIOTERAPIA: Es el tratamiento con radiaciones ionizantes con tecnologías como radioterapia de intensidad modulada (IMRT). Estos tratamientos usan computadoras y técnicas especiales para enfocar la radiación en el cáncer y limitar el daño a los tejidos normales adyacentes. El paciente se acuesta en la camilla y tiene que permanecer quieto durante los minutos que dura la administración de la radioterapia. La radioterapia NO es un tratamiento doloroso.
Actualmente la Clínica de Radioterapia Siglo XXI cuenta con la tecnología y experiencia para tratar este tipo de enfermedades, garantizando la protección de órganos y tejidos circundantes, brindando así una mayor calidad de vida para el paciente.
Para tratar el cáncer gástrico la radioterapia se puede utilizar de diferentes maneras:
Después de la cirugía que se denomina radioterapia adyuvante se puede usar para destruir los remanentes pequeños que no se pueden extirpar con la cirugía. La radioterapia se puede acompañar de quimioterapia para prevenir o postergar la recurrencia y aumentar su efectividad.
Con menor frecuencia se puede administrar antes de la cirugía de forma neoadyuvante con quimioterapia para tratar de reducir el tamaño del tumor y facilitar la cirugía. La decisión de administrar la radioterapia de forma pre o postoperatoria depende de una serie de factores que varían de un paciente a otro y será decidido por el médico tratante.
Como tratamiento paliativo, la radioterapia es eficaz para desacelerar el crecimiento, controlar el dolor y aliviar los síntomas del cáncer gástrico avanzado. En esta situación, se suele administrar sola, sin quimioterapia.
